

I should be grocery shopping. My poor kids lunches were pathetic because of my lack of grocery shopping yesterday. No regrets we were having fun at the beach. Still a bagel with cream cheese, banana and slim jim is not exactly the lunch my kids were each hoping for.

I should be cleaning my house. At least 3 loads of laundry are in a pile in laundry room. A nearly fruitless search for socks this morning was not a great way to start the day. The dishes in the sink aren’t going to wash themselves and it is never good when the cat can chase around fur bunnies due to lack of vacuuming. Again – no regrets the beach was amazing.
I should be organizing closets and the garage – can’t list my house for sale in its current state. It would be bad for potential buyers to have to step lightly around ironman action figures, rogue legos and stacks of who-knows-what. Eh – I’ve got a bit more time before I need to list the house. It’ll all come together even if it takes a few pots of coffee and some stress eating (i never do that).
What have I been doing all morning? Glad you asked – well you stuck around this long to find out about glucagon so I assume you are slightly interested.
So my Middles has been requiring shots of Novalog more and more frequently. He had been using only Lantus (long acting insulin) to manage his diabetes. Unfortunately his pancreas is clearly pooping out sooner than we had hoped. During the Thanksgiving break he was receiving 2-3 shots of fast acting insulin due to after meal spikes (the high carb count meals during the break were not helpful).
Today he returned to school. His morning BG (blood glucose) was 155. Not excellent but not shabby considering the 457 he went to bed with (received novalog to correct that number). He ate a 30grams of carbs for breakfast and off he went. I told him to text me his numbers 2 hours post meal and if he was above 250 I would come give him a shot of novalog. (He has not been using fast acting insulin at school and thus no doctors orders are on file and he hasn’t been carrying insulin with him)
At 9:15am I get the text: “Im 401 please bring me insulin.”
I cancel a coffee meet-up and head off to the school. I give the boy 1.5 units of novalog, remind him to drink water and watch his sugars then send him off to class.
Seeing as I had just given him fast acting insulin and he is still very much honeymooning (a time after diagnosis where the patient still produces some insulin so less artificial insulin is required) I wanted to leave the school office staff with a glucagon kit.
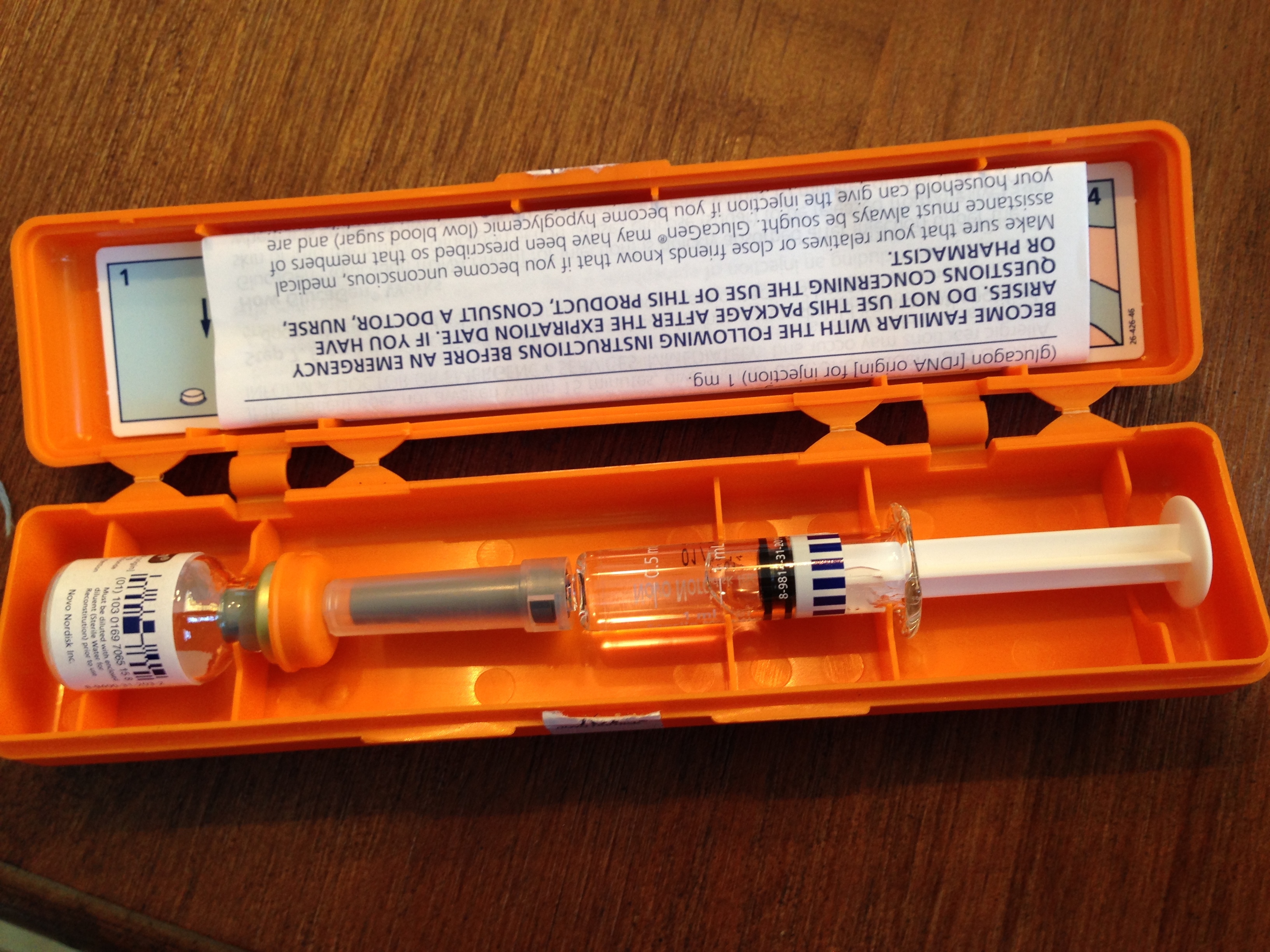
A Glucagon kit is an emergency kit for people with diabetes. Similar to an EpiPen used by those with severe food allergies only it isn’t a pen – it is a vial of a powdered form of synthetic glucagon – (a human hormone that triggers the liver to release glucose) and a syringe filled with distilled water. To use the glucagon kit one must inject the water into the vial of powdered glucagon, swish to mix and refill syringe with liquified mixture, then inject into person with diabetes. This is normally only done if the pwd is unconscious or having seizures do to a severe hypoglycemic episode (hypoglycemia is caused when there is too much insulin and too little sugar in the body – it can be deadly). A side note – glucagon can and sometimes is used in small injections for a pwd that is experiencing a very low blood sugar but is not unconscious or having a seizure – or if the pwd is very low but can not eat or drink any sugary substance.
Ok – moving on now that any newbies know what a glucagon kit is and why it is used.
I anticipated the office staff (there is no nurse on school property other than on Fridays) having an idea of what a glucagon kit is and who should be contacted if it is required.
I got blank stares. The two office staffers knew nothing about glucagon. Not only had they never seen one they didn’t believe any staff on campus knew what they were or if any were trained to use the emergency kit.
Seriously? My son is not the only cwd at the school. There are at least 3 others that I know of, maybe more. Certainly someone in the school knows about diabetes and glucagon and emergency diabetes care.
A bit of back story. California as a whole sucks big time at diabetes in school. There are some schools and some districts that are better than others at providing support. But up until July of 2013 no non-licensed person (meaning no one that wasn’t a certified nurse) could assist in insulin injections. In July the CA supreme court ruled that it was now legal for non-medical staff to assist in insulin administration. Prior to the ruling parents of cwd who were not independent (meaning they managed their diabetes without supervision at school) would have to go to their child’s school and assist their child or their child would not get insulin all day even for meals. CRAZY right? The new law was supposed to ensure that schools would have at least 1 or more staff members willing and able to assist in determining insulin amount, injecting insulin, and overseeing care in general. Our school district basically hasn’t decided if they want to adhere to the law. It seems they think it is a voluntary law. Anyway I’m digressing – this post isn’t so much about the laissez faire way the district approaches the insulin law it is about emergency care.
Even before the recent Supreme court ruling schools have been required to have staff trained in emergency care – i.e glucagon.
It isn’t enough to train staff. All school staff should be aware of who is trained in glucgon administration. So imagine my shock to learn that the office staff – the staff that have to deal with medical emergencies have no idea if anyone is trained or who those staff members would be. Who’s in charge of training staff and disseminating the information? Well it falls on the nurse. The nurse that is only at the school 1 day a week. It should also fall on school administration. This school nurse has dropped the ball. There was no list of people trained.
The very sweet and kind office staff member that was fortunate enough to deal with a flustered mom this morning (thats me) was doing her best to find the information and help rest my nerves. She did ask me to explain the glucagon to her and I did. I was sure to explain that a person cannot be harmed by glucagon. The only thing glucagon can do is a save a life. It isn’t like insulin I say. It is true insulin can kill a person if administered incorrectly and I am not asking for anyone to inject my son with insulin (even though its the law and I have ever right to ask that). She listened to the instructions, asked questions and assured me my son would be safe. I assured her he would never likely need the glucagon but felt better she at least listened to my explanations. I assured her I would bring in an old glucagon and train any and all willing how to use it. (Not my job but better me than a nurse that can’t be trusted to do her job). (blimey I used the word ‘assured’ a number of times there.)
The staffer called me a bit after I left to let me know that the principal, assistant principal and counselor were familiar with glucagon. She didn’t say when they were last trained. I feel better knowing that the school does have 3 trained staff members. Still it would be helpful if other staff – the ones most likely to get the emergency call from a panicked teacher – knew who was trained and that there are emergency procedures to follow in addition to calling 911.
I had not asked at Middles school who was trained prior to today because until today my son was not using fast acting insulin at school. However – I have also not asked at my other two children’s schools. They do take fast acting insulin daily at school. What if the same is true at the other two schools – no one knowing who is trained – are there people trained? I took the nurses word for it – When she said she trained 3 people I believed her. Let’s assume she did train 3 people in each school – does anyone at those schools know who is trained? Do teachers and office staff know emergency protocol for cwd?
I miss my Texas schools. I miss the way every staff member at the schools knew which kids had diabetes, which had severe food allergies and what actions to take if there was an emergency whether it was on the playground, cafeteria, classroom, library or gym. Everyone knew the damn protocol. I wish schools across the country would recognize the importance of educating all staff regarding medical emergencies. With food allergies and Type 1 diabetes on the rise – both are increasing by 3% or more each year – schools should be prepared.
I spend hours every week tweaking insulin dosages, counting carbs, changing pump sites, charging meters, checking late night blood sugars, learning about new technology, new diabetes management methods, etc – HOURS – and my kids are right there with me much of the time. All this effort and planning should not go to hell in a hand basket the moment any of my kids step foot in a school.
So my advice – just in case like me – you have put your trust in others and believed them to be working in the best interest of your child. (Note – when my daughter was dxd I was at the school often to ensure every base was covered – I wasn’t so laissez faire myself back then) – double check who is trained in glucagon at your child’s school. Who knows who is trained? What is the emergency protocol for your child’s school? Even if you did this when your child began kinder or when he or she was first dxd – if it is a new school year – maybe check into it. Staff changes and sometimes things like emergency protocols for kids with chronic illness are not passed on to new staffers (that is the case at my sons school).
Oh my – I was a bit wordy today. Here is a cute cat picture for your time. Wish it wasn’t of my cat sleeping – tried to catch her playing with fur bunnies but that didn’t happen. Mostly she sleeps. It must be hard being a cat.


Interesting that you write this because I was thinking about this from the other side a few days ago–as in, what would be the reactions of the staff at the daycare I work at if we had a kid in our care with diabetes to all the intricacies of management. (For once, like asthma care, I’d be the one ahead of the learning-curve because I hang with all the lovelies in the DOC).
Of course, my question becomes then [especially after just writing a paper about life-threatening food allergies and the psychosocial effects on kids and families], given the crap system we have here for in-school medical care, how many parents have put their own careers on hold because of inadequate provision of care in schools? The US has a better system of accommodation protection, I think, than Canada [don’t quote me on that], even if the system changes everywhere.
In Manitoba, the education system funds nursing care for students who need it–one thing I do like, though, is that we have a program called Unified Referral and Intake System [or URIS]. Beyond if a student needs care from a nurse in school, the URIS nurse is assigned to a certain school division/part of a school division to provide training to staff in that building (I don’t know if it is ALL staff, but would certainly be all who have regular direct contact with the student), meaning everyone receives identical training and identical action plans to follow [I’ve only seen asthma and anaphylaxis training implemented; when I started we had a kid with epilepsy, but he left once I was there for six weeks and since those were my orientation-type weeks, I was never solely providing care for him]. Changes to a student’s plan are made through the URIS nurse who then re-trains staff if any changes occur. So, as the daycare I work at is inside a school, we receive all of the same training as the school does.
As I’ve said before, I DO like the new law in California so long as parents feel their child is receiving adequate care–our system details that certain aspects of care [including injections that are not via autoinjector] have to be given by a RN. I understand, but only to an extent–something like glucagon? Like you’ve said, if it’s given at the wrong time, little harm done–but if it’s not? Bad news. Given our system, I’d *hope* that the parent could consent for the training nurse to instruct staff on how to use glucagon when minutes count–the device shouldn’t matter, education should. As I sit here with both an EpiPen and an Allerject [Auvi-Q] trainer beside me, for both the sake of people with diabetes, and parents of kids with diabetes, and anybody who knows them, that they’re able to figure out the whole stable-glucagon thing soon and an autoinjector is available soon–like epinephrine, it just makes so much freaking sense, and, also like epinephrine, little harm will be done if glucagon is used at the wrong time. Because it doesn’t matter if three people in the building are trained, it matters that care can be given as quickly as possible–it makes no sense to me that school administration doesn’t seem to understand this.
And as for jumping on them about their knowledge–better late than never, right?
LikeLike
Holy novel – AWESOME.
It saddens me to learn of parents that have had to put their carriers on hold but still many do it, not just for diabetes either – so many other kids that have cognitive or physical differences that require constant care. Its what parents do because of love for their child.
Curious that glucagon in Manitoba and other areas of Canada is considered non-autoinjector (I mean it is non-autoingector) thus not able to be utilized by non-health professionals. Thankfully it is considered emergency treatment here and can be administered by non-health professionals.
I think it comes down to the scariness of it all. Asking school staff to be responsible for the physical well being of children that take a drug daily that could kill them is scary.
I just think with the proper education and training it would become less scary and more staff would be willing to assist.
Thankfully we will be leaving this district soon. hoping WA schools are a bit more educated.
LikeLike
Blessings to you and your son.
btw, Glucogon doesn’t contain glucose. Glucogon is a hormone to force the liver to release stored glucose instead.
I have two t1s and I’ve never been trained to use it and don’t even have any in the house. We’re told the paramedics will carry it and that’s that.
LikeLike
Hey there Angela. Thanks for the reply and alerting me to my mistake – thats what I get for trying to write a post while still fuming from my interaction with the school. I have updated the post so as to not confuse people.
I meet many parents that have not been prescribed glucagon or have not ever renew their prescriptions since diagnosis. I think at the hospital we are handed so many new things that the glucagon gets tossed in the mix with little explanation. Still I renew them each year. I have given many away to schools to use for training but I bet I still have a dozen or more around the house. True the paramedics carry them but still I like the idea of having them handy and having them at the schools. I just feel better having them around and in my purse.
LikeLike
I would trade a day at the beach for laundry & cleaning anyday. What great memories you’re making with your kids!
So sad that so many schools seem to be so unsupportive. Even worse, many seem to have no interest in changing.
One note about paramedics & glucagon: it’s really best to check with the EMTs in your area. Here, glucagon is not carried in the ambulance, nor is it administered. My BIL, a professional firefighter in a nearby city, says it also is not carried or used by paramedics there. The reason? They can’t be sure it will work. The patient could have had numerous hypos during the day, which would render the glucagon ineffective. Dextrose is given via IV instead, because the results are more reliable.
LikeLike
good to know about paramedics. I mean it isn’t like I tell people how to do their job 😉 but I could see myself just yelling give him glucagon!
LikeLike
As much as I don’t like living I Texas, I am very thankful for how well-advocated our kiddos are in school here. There has been talk about moving to CA, and my response is, “no way”. Because of exactly what your post was about.
LikeLike
oh Jo – don’t let the schools lack of D care keep you from moving here. It really is a good place to live. We would stay happily if the cost of living wasn’t so ridiculous.
LikeLike
Sorry to hear that the school staffs there know so little about CWD care. I find it baffling that Texas schools would be so good, and Middles school isn’t. I guess it is the individual states that make up their own rules. Why isn’t there a national policy that would apply throughout the US? I know, too much to ask for. I know you have three CWD’s now, and you have never had to use a glucagon kit. That is good. I hope you never need one.
I have been keeping in touch with Christel on Facebook. She has joined a group called “Diabetes Mastermind”. The administrator of the group is Dr. Sybil Kramer, an endo in the Boston area. She is very good, and volunteers some time to answer questions, and present some very interesting info. You might want to message Christel for her impression of the group.
LikeLike
Thanks Richard. I have learned that WA (where we are moving) is hit or miss too with D care in schools. It is clearly a state decided and even district thing. It would be good if there was a national standard.
Ill checks with Christel about the Mastermind group. Thanks again and yes – I too hope I never need glucagon.
LikeLike
Wow, it still amazes me that schools elsewhere do such a poor job with medical stuff. Texas does rock at that pretty good. I’m sorry you had to deal with all that!
I have a high school classmate that is a nurse in CA. When that was all going down, she posted about it on fb. I wasn’t going to comment, but a mutual friend tagged me and asked my opinion. I basically said it doesn’t require a nurse or any medical training to administer insulin (or glucagon). I learned it in ICU in a 5 minute lesson. She (the nurse) never commented back.
LikeLike
I have found that most nurses in CA don’t like to hear that a nursing degree isn’t necessary to do diabetes care. The unions here really brainwash them and they are fighting for jobs. I get that but if the nurses really cared about our kids they wouldn’t fight it so hard.
LikeLike